DESCRIPTION
The shoulder joint is a ball and socket joint, with the humeral head (upper arm bone) as the ball and the glenoid as the socket. The glenoid (socket) is a shallow bone that is encircled with tissue called the labrum. (See Figure 1) The labrum acts as a stabilizer for the head of the humerus as it deepens the socket in which the humerus rests.
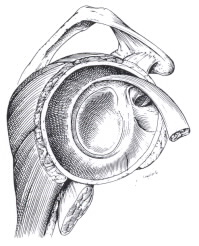
Fig. 1. Intact labrum and biceps tendon.
Labral tears can be classified based on where the tears are located. If the superior or upper portion of the labrum is detached it is classified as a SLAP tear. (See Figure 2) If the lower labrum is separated from the bone it is classified as a Bankart tear. (See Figure 3) Labral tears can occur in conjunction with shoulder impingement syndrome or rotator cuff inflammation.
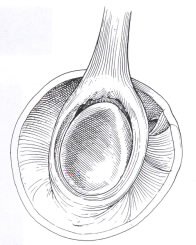
Fig. 2 Superior Labral tear or SLAP tear
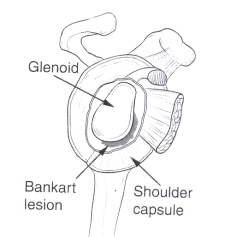
Fig. 2 Superior Labral tear or SLAP tear
PREVENTION AND RISK
Throwing athletes and overhead athletes such as swimmers are at increased risk for having labral.
Labral tears can cause increased motion within the shoulder joint, which can cause inflammation elsewhere in the shoulder.
SYMPTOMS
Patients may notice anterior, posterior or lateral shoulder pain. Patients may also notice pain with throwing or overhead activities.
TREATMENT)
Treatment involves both surgical and non-surgical options. An MRI may also be obtained to evaluate the labrum, shoulder joint and rotator cuff tendons.
Non-surgical treatment is recommended prior to surgical intervention.
NON-SURGICAL TREATMENT
1. Rotator cuff strengthening
Exercises strengthen the muscles and tendons surrounding the shoulder joint and act as secondary stabilizers. They also decrease inflammation in the rotator ruff tendons. These exercises can be done at home, at a gym or with a physical therapist. (See Fig 4)
2. Anti-inflammatory medications
It helps decrease inflammation as well as treat pain.
3. Cortisone injection
Applied into the subacromial space may decrease inflammation and overall shoulder symptoms in combination with Rotator Cuff Exercises.
SURGICAL TREATMENT
Shoulder surgery is always done via arthroscopy (surgery guided by video imaging as opposed to open surgery). Surgery stabilizes defects in the labrum. Labral repair occurs with placement of a small anchor into the glenoid. Suture is attached to the anchor and used to secure the tissue back to the glenoid.

Pre Labral Tear sugery
Post Labral Tear repair surgery
REHABILITATION
Rehabilitation exercises focus on strengthening the shoulder, specifically the rotator cuff, and upper back. Rotator cuff strengthening exercises include internal rotation, external rotation and supraspinatus. Exercises can be done with therabands, hand weights or cable pulleys at a gym which are adjusted to the appropriate height.
Each exercise should be done PAIN-FREE, and for 3 sets of 20 repetitions. If the patient is unable to do 20 reps, then either the weight or the resistance should be decreased.
See Fig 4-16.
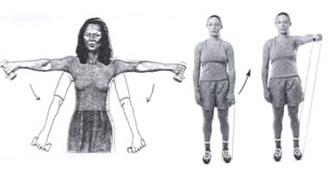
Exercises with hand weights and therabands.
Always have your thumb pointing to the floor, your arm out 45 degrees,
and keep your arm below shoulder height.
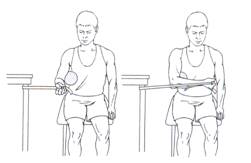
Fig 5: Internal Rotation. Hold a small ball or towel between arm and side
and slowly rotate forearm across body. Return to start and repeat.
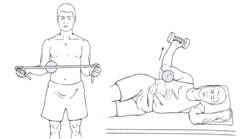
Fig 6: External Rotation. Hold a small ball or towel between arm and side
while holding a weight or band; slowly rotate forearm away from side. Return to start and repeat.

Fig 7: Scapular Elevation, Shrugs. Stand with arms at side in straight standing posture, shrug or raise shoulders up towards ears. Briefly hold, return to start and repeat. A hand weight can add difficulty.
Secondly, pull shoulder blades or scapula together in the back, hold, and then relax shoulders forward. Repeat.

Fig 8: Scapular Protraction. Lie on back holding a hand weight.
Keep elbows straight push hands up towards the ceiling, hold, return to start and repeat.
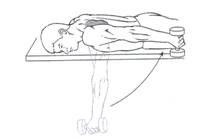
Fig 9: Shoulder Extension. Lie on stomach and with arm hanging off the side of the bed.
Hold a hand weight and slowly raise your arm up until it is level with side and next to body,
hold, slowly return to start and repeat.

Fig 10: Shoulder Flexion. While standing holding a hand weight or resistance tubing, slowly raise arm overhead, hold, slowly return to start and repeat. Motion should be pain free. Avoid shrugging the shoulder.

Fig 11: Scapular Retraction. Anchor tubing to a fixed object and hold ends of tubing in each hand.
Squeeze and pinch your shoulder blades together, pulling your arms back.
Hold, slowly return to start and repeat.
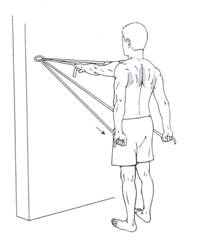
Fig 12: Shoulder Extension. Anchor tubing to fixed object and hold ends of tubing in each hand.
Slowly pull hands down to the side while squeezing shoulder blades together.
Hold, slowly return to start, and repeat.

Fig 13: Horizontal Abduction. With a hand weight, lie on stomach and start with the arm hanging down.
Keep the elbow straight, slowly raise arm up and out from side. Hold, slowly return to start and repeat.
With a band, hold one end in each hand in front of body. Keep elbows straight, pull arms apart, or out to the side at shoulder height. Hold, slowly return to start and repeat.

Fig 14: Scapular Retraction and External Rotation. If using a weight lie on stomach, with arm out to the side hanging down with elbow bent at 90 degrees. Upper arm should be supported by the bed. Turn and rotate arm towards the ceiling while keeping the elbow bent at 90. Squeeze the shoulder blades together, hold, slowly return to start. If using a band, bend each elbow at 90 degrees at shoulder height and squeeze shoulder blades together. While squeezing shoulder blades, raise hands above shoulder height as shown. Hold, slowly return to start and repeat.

Fig 15: Scapular Retraction and Elevation. Hold one end of the band in each hand at shoulder height. Squeeze and pinch shoulder blades together and while keeping both arms straight slowly raise arms overhead. Try to keep thumbs in a ‘thumbs-up’ position. Hold, slowly return to start and repeat.
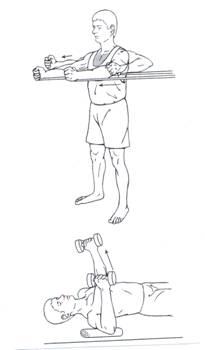
Fig 16: Horizontal Adduction. With weights- lie on back holding weights with elbows bent. Slowly raise arms towards ceiling straightening elbow. Hold, slowly lower and repeat. With bands anchored behind, slowly push arms out in front straightening elbows. Hold, slowly bend elbows and repeat.
