
Pain in the front of the knee is a very common complaint. The pain usually originates from the tissue around the kneecap including the tendons, bones and cartilage surfaces. These tissues are put under high forces during many common activities and especially during sports. Running, jumping, hiking, squatting and lunging can place up to six times an individual's body weight through these tissues. Repetitive high loading eventually leads to tissue breakdown and subsequent pain. Women are more susceptible to these problems because their kneecaps are smaller and often "track" abnormally. High forces in a small distribution area leads to painful "chondromalacia"(chondro=cartilage; malacia=bad).
The cartilage surfaces behind the kneecap are the thickest in the entire human body and usually begin to wear out after the age of 15. Almost all people have evidence of cartilage damage on kneecap cartilage when we perform arthroscopic surgery. It is interesting to note however that while the pain from chondromalacia is the most common complaint of people between the ages of 15 and 60, these complaints usually disappear after age of 60. In addition, most persons with chondromalacia do not have symptoms.
While the cartilage surfaces do not have any nerve endings, all the tissues around the kneecap cartilage (including the bones) do have nerve endings and can therefore produce pain. The most common finding on examination is tenderness to touch around the kneecap or patella. There can be swelling and often there is grinding with bending or squatting. Often people can hear grinding coming from their knees when squatting and stair climbing.
The most common medical finding is damage to the cartilage behind the kneecap (patella). The cartilage covering, or articular cartilage, that covers the knee cap bone is the thickest cartilage covering in the entire human body. The reason the cartilage covering in this area is so thick is because the knee cap takes more pressure per unit of area than any other joint in the body. With squatting and lunging activities up to six times the body weight is placed into the small bone of the knee cap and the cartilage. With activities this cartilage can begin to breakdown and produce pain.
The primary treatment of anterior knee pain or chondromalacia of the patella is a strengthening program of the quadriceps muscle. Strengthening of the quadriceps muscle when done properly often results in approximately 90% cure rate for this condition. The reason that strengthening of the quadriceps muscle is effective is that it takes the pressure away from the knee cap cartilage and puts it into the muscular tissue. Also strengthening of the quadriceps muscle assures that the kneecap is tracking properly and distributing the load evenly inside the knee cap-thigh bone joint.
Exercises involve strengthening-stretching of the quadriceps muscle. All strengthening of the quadriceps muscle should be done within the range that keeps pressure on the kneecap low. This range is between full extension (the knee is completely straight) to approximately 45 degrees of bending of the knee. The exercises should be done with lightweight and high repetition in three sets of 20, or sets of 30 are appropriate. There should be no pain during the exercises. After the exercise program ice should be applied to the front part of the knee for approximately 10-20 minutes. Anti-inflammatory medicines are also very useful and may be taken on a daily basis. Exercises can be performed on a daily basis, but should be performed at least three times a week. Activities that cause pain should be modified or abandoned temporarily until the pain resolves. With an exercise program most people are able to resolve the pain and return to full activities without difficulty within a three to six month period of time
Quadriceps Exercises
- Leg Press
-
Leg Extension
-
Squats
Hamstring Exercise
-
Hamstring Curl
-
Calf Exercises
-
Calf Raises
Other
-
Bike (seat elevated)
-
Stairmaste
-
Elliptical Trainer
-
Rollerblade
If exercise and strengthening are not enough to decrease symptoms lubrication or viscosupplementation injects may be of benefit.
Within the knee joint synovial fluid is highly viscous which provides a friction-free environment. Hyaluronic acid (HA) which is present in our synovial fluid is also found in most body tissues. In a healthy adult, synovial fluid HA has a molecular weight of 4-5 million. As a result of this large size HA molecules entangle, forming coiled configurations which in turn provide elasticity and viscosity to synovial fluid. HA also binds to proteoglycans to stabilize the structure of the articulate cartilage. In patients with OA, the molecular weight of the HA decreases causing the synovial fluid to become less viscous thus leading to increased friction and abnormal joint movement.
Lubrication or Hylagan injections provide the joint extra lubrication and shock absorption, as well as decrease friction or rubbing within the joint which may slow the progression of osteoarthritis. However, of all the patients who receive Hylagan injections, only about 50% have symptomatic relief. One injection is given into the knee each week for three weeks and may be repeated as soon as 6 months. Up to five injections may be given, but studies have shown no difference in symptom relief after 3 or 5 injections.
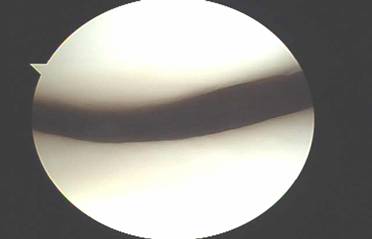
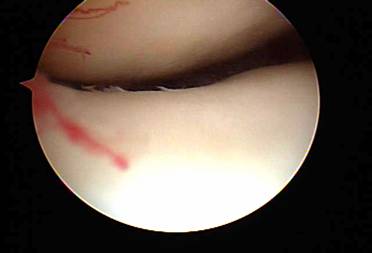
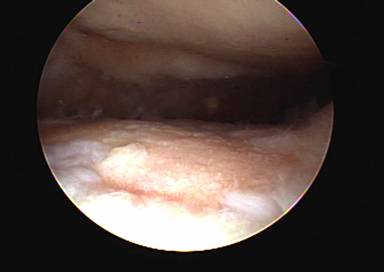
When exercises fail to improve the knee then surgery may be indicated if the symptoms are significant enough to alter activities. The most common arthroscopic surgical procedures to treat chondromalacia include chondroplasty and microfracture / abrasion procedure. A chondroplasty involves smoothing out roughened surface cartilage which can decrease friction forces on the surface cartilage and decrease symptoms of chondromalacia. An abrasion or microfracture is most useful when there is a small contained area of exposed bone or complete loss of surface cartilage. During this procedure the bone is tapped with a pick-type tool which causes bleeding in the area of exposed bone. This blood from deep inside the bone carries stem cells which can cause the bone to grow a scar type cartilage. This scar cartilage has been shown to be very effective in reducing knee pain in several orthopedic studies.
While surgery can be effective in reducing symptoms it must also be accompanied with non-surgical treatment such as decreasing overall body weight, increasing muscle strength of the leg muscles, and if needed activity modification. If these treatment options are not adequate in resolving pain or returning the patient back to all activities other more aggressive surgical options are available.
 />
/>
 />
/>
 />
/>