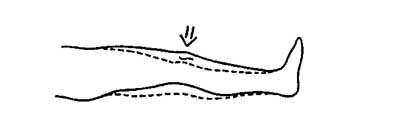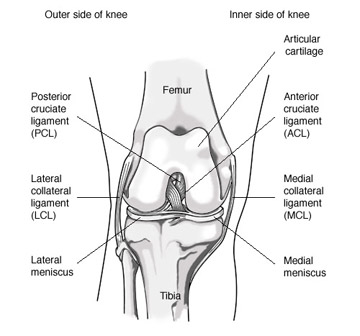
The medial collateral ligament (MCL) runs on the inside of the knee from the thigh bone (femur) to the shin bone (tibia) along the inside of the knee joint. The MCL prevents the knee from buckling inward.
Most MCL injuries occur during sports when the knee is forced inward.
Many times injuries can be prevented by maintaining proper strength, conditioning, and body mechanics. However injuries to the MCL are usually a result of medial or inward pressure as a result of contact in sport and can not be prevented.
With a MCL injury patients usually note pain and tenderness on the inside of the knee joint. Pain with full straightening of the knee may occur. Patients also may note feelings of instability and knee stiffness. The MCL runs on the outside of the knee joint so a large amount of swelling in the joint is not common.
MCL injury is classified with Grade I through Grade III injury. Grade I refers to a mild sprain, Grade II moderate sprain and Grade III severe sprain / tear of the MCL.
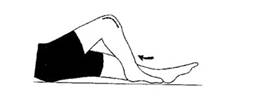
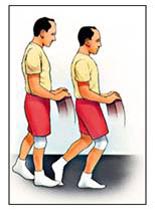
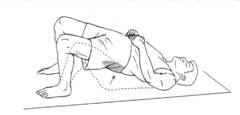
After an acute episode, the patient will be initially treated with RICE (rest, ice, compression, and elevation). A hinged knee brace and crutches may be warranted based on severity of injury and/ or degree of instability. Ranges of motion exercises are important to restore flexibility, and strengthening the quadriceps stabilize the knee joint. Physical therapy can be very helpful.
MRI may be useful to evaluate for any other knee injuries.
Most patients with a MCL injury will do very well with rehabilitation and will not require surgery. Patients who may require surgery will continue with instability despite rehabilitation.
If patients failure to improve after nonsurgical treatment, a surgical reconstruction of the MCL may be indicated. This surgery is done through a small open incision where a new ligament is fixed into place.
The vast majority of patient with injuries tot heir MCL will not require surgery and will be able to fully rehabilitate with nonsurgical treatment and rest.
All exercises should not cause increased pain or swelling. Work up to at least 3 sets of 20 repetitions, at least 4 days a week. See Fig 2-7.